

Stage IA Lung Cancer Has a 90% Survival Rate. Most Patients Never Get the Chance
Juan Vegarra
Add paragraph text. Click “Edit Text” to update the font, size and more. To change and reuse text themes, go to Site Styles.
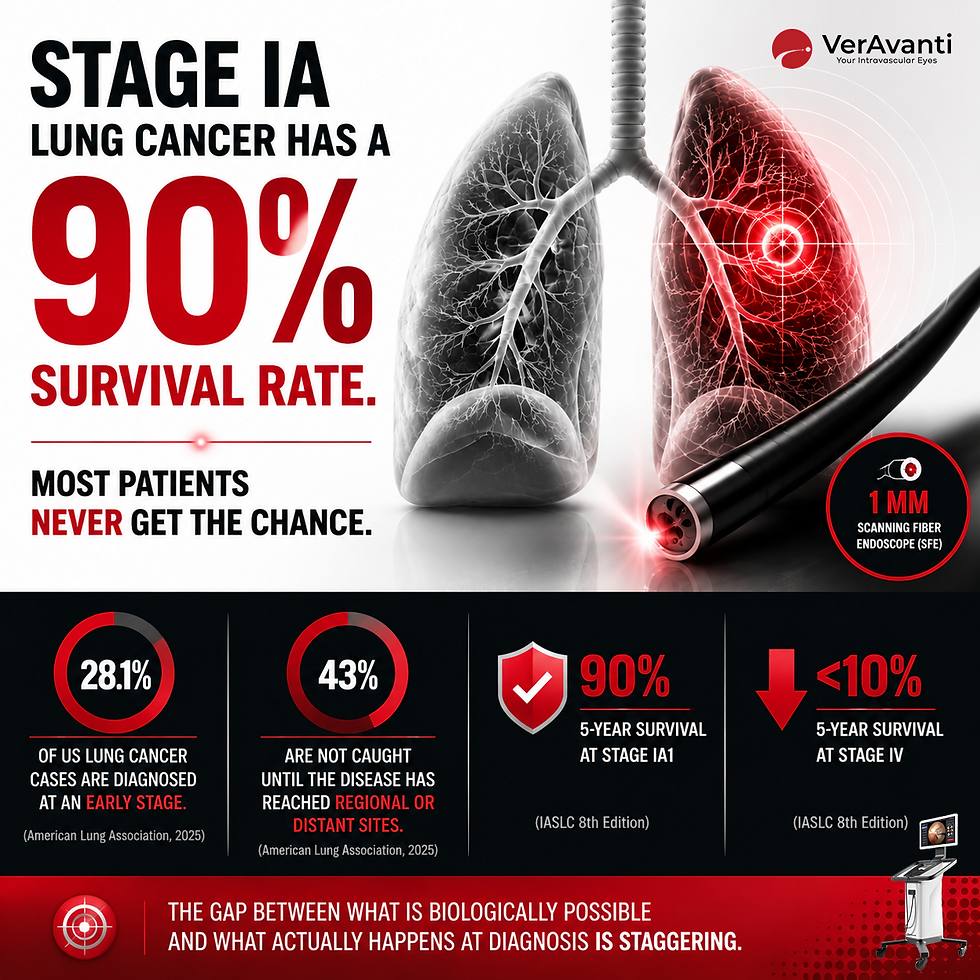
Caught at Stage IA1, lung cancer has a 5-year survival rate of approximately 90%. Caught at Stage IV, that number drops below 10% [1].
That is the entire story. Everything about lung cancer outcomes, every screening program, every diagnostic algorithm, every device VerAvanti is building, exists to move patients from the second number to the first.
Today, only 28.1% of US lung cancer cases are diagnosed at an early stage. 43% are not caught until the disease has reached regional or distant sites [2]. The gap between what is biologically possible and what actually happens at diagnosis is the largest unsolved problem in thoracic oncology.
It is also, increasingly, a tooling problem.
The numbers behind the cliff
The American Cancer Society projects 226,650 new US lung cancer cases and 124,730 deaths in 2025, accounting for more than one in five of all cancer deaths and roughly 2.5 times the mortality of colorectal or pancreatic cancer [3].
Survival depends almost entirely on stage at diagnosis. Under the IASLC 8th edition staging system, 5-year survival for NSCLC is approximately 90% at Stage IA1, 85% at Stage IA2, 80% at Stage IA3, and falls below 10% at Stage IV [1].
Low-dose CT (LDCT) screening reduces lung cancer mortality by 20% in high-risk adults per the National Lung Screening Trial, and by 24% in men with a 33% reduction in women per the NELSON trial [4, 5]. Yet only 18.2% of screening-eligible US adults were screened in 2022 [2]. The result is a growing population of indeterminate peripheral nodules sitting on CT scans, and a diagnostic toolkit that often cannot reach them.
Why the tools cannot reach the disease
Most early-stage lung cancers form in the lung periphery. The tracheobronchial tree branches through roughly 16 generations before terminating in bronchioles measuring approximately 1 mm or less in diameter [6].
The tools designed to see those nodules are an order of magnitude too large.
Conventional flexible bronchoscopes have outer diameters of 4 mm to 6 mm [7]. Ultrathin bronchoscopes, defined as those with outer diameters of 2.8 to 3.5 mm, can advance further into peripheral airways but still cannot enter the small distal airways where many of the most clinically important nodules sit [8, 9].
The diagnostic consequences are well documented:
Conventional flexible bronchoscopy under fluoroscopic guidance achieves diagnostic yields of 10% to 50% overall and approximately 33% for peripheral lesions less than 20 mm in diameter [10].
Even with electromagnetic navigation bronchoscopy (ENB), real-world diagnostic yields range from approximately 54% to 73% depending on technique and lesion characteristics [11, 12].
Bronchoscopic biopsy of nonmalignant findings carries a 23.7% false-negative rate at 2-year follow up [13].
Patients with inconclusive bronchoscopy results face limited options: a repeat bronchoscopy, a CT-guided transthoracic needle biopsy with a meaningful pneumothorax risk, surgical biopsy, or active surveillance that delays treatment.
The forward-looking view problem
Every existing intraprocedural imaging modality has a structural limit. Fluoroscopy provides 2D guidance with ionizing radiation. Radial endobronchial ultrasound confirms lesion contact but provides no real-time visual context. OCT and IVUS provide cross-sectional views but no forward field of view. Conventional bronchoscope cameras stop at the airways they can physically enter.
What clinicians do not have is a sub-millimeter device that delivers a real-time, forward-looking, full-color view of the airway as it advances toward a peripheral target.
Where the SFE will fit
VerAvanti is developing the Scanning Fiber Endoscope (SFE) as a 1 mm diameter, radiation-free, full-color imaging platform. A single resonating optical fiber paired with red, green, and blue laser illumination produces high-resolution video through a wide forward field of view.
The device was originally engineered for intravascular imaging. Its form factor and forward-looking optics make the peripheral airway a natural area of evaluation. A device that can advance distal to the reach limits of current bronchoscopes, with real-time visual confirmation of the airway it is traversing, has the potential to change the workflow for indeterminate peripheral nodules.
What's next
The clinical problem is clear. The data is consistent across the American Lung Association, the American Cancer Society, and the peer-reviewed bronchoscopy literature. Closing the gap between Stage IA and Stage IV at diagnosis will require imaging tools sized to the anatomy where the disease begins.
VerAvanti is pursuing FDA 510(k) clearance for an initial cardiovascular indication anticipated in the second half of 2026. Peripheral pulmonary applications are under evaluation as an adjacent indication.
References
Goldstraw P, Chansky K, Crowley J, et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2016;11(1):39-51. doi:10.1016/j.jtho.2015.09.009
American Lung Association. State of Lung Cancer: 2025 Report. November 2025. https://www.lung.org/research/state-of-lung-cancer
Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A. Cancer statistics, 2025. CA Cancer J Clin. 2025;75(1):10-45. doi:10.3322/caac.21871
National Lung Screening Trial Research Team. Reduced Lung-Cancer Mortality with Low-Dose Computed Tomographic Screening. N Engl J Med. 2011;365(5):395-409. doi:10.1056/NEJMoa1102873
de Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N Engl J Med. 2020;382(6):503-513. doi:10.1056/NEJMoa1911793
Weibel ER. Morphometry of the Human Lung. Springer-Verlag; 1963. Standard reference for tracheobronchial branching anatomy and terminal bronchiole dimensions.
Chen AC, Pastis NJ, Folch EE, et al. Robotic Endoscopic Airway Challenge: REACH Assessment. Ann Thorac Surg. 2018;106(1):293-297. doi:10.1016/j.athoracsur.2018.01.051
Oki M, Saka H, Ando M, et al. Ultrathin Bronchoscopy with Multimodal Devices for Peripheral Pulmonary Lesions: A Randomized Trial. Am J Respir Crit Care Med. 2015;192(4):468-476.
Olympus Medical Systems. BF-MP190F/MP290F Ultrathin Bronchoscope Specifications (3.0 mm distal-end outer diameter).
Gould MK, Donington J, Lynch WR, et al. Evaluation of Individuals with Pulmonary Nodules: When Is It Lung Cancer? Diagnosis and Management of Lung Cancer, 3rd ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2013;143(5 Suppl):e93S-e120S.
Folch EE, Pritchett MA, Nead MA, et al. Electromagnetic Navigation Bronchoscopy for Peripheral Pulmonary Lesions: One-Year Results of the Prospective, Multicenter NAVIGATE Study. J Thorac Oncol. 2019;14(3):445-458.
Khandhar SJ, Bowling MR, Flandes J, et al. Electromagnetic navigation bronchoscopy to access lung lesions in 1,000 subjects: first results of the prospective, multicenter NAVIGATE study. BMC Pulm Med. 2017;17(1):59.
Outcomes and Clinical Practices in Follow-Up of Nonmalignant Pulmonary Nodules After Bronchoscopic Biopsy. CHEST Pulmonary. 2024;2(3):100078. doi:10.1016/j.chpulm.2024.100078
(The Scanning Fiber Endoscope (SFE) is an investigational device. It is not cleared or approved by the U.S. Food and Drug Administration and is not available for sale. Clinical applications referenced beyond the initial cardiovascular indication are under evaluation.)