

From Rigid Tubes to Real-Time Views
A Deep Dive into Endoscopy and Intravascular Imaging Since 1980
Juan Vegarra
Add paragraph text. Click “Edit Text” to update the font, size and more. To change and reuse text themes, go to Site Styles.
The desire to visualize the hidden workings of the human body without resorting to major surgery has been a defining goal of medicine for centuries. While the earliest attempts at endoscopy the practice of viewing the body’s interior, date back to the 19th century with Kussmaul’s rigid esophagoscope, the period since 1980 represents a technological and clinical watershed.
This era saw the transition from cumbersome, fiber-optic bundles to high-definition digital cameras, fundamentally transforming diagnostic and therapeutic capabilities across every medical specialty. Crucially, this evolution spawned a specialized, revolutionary field: intravascular imaging (IVI).
This article establishes a comprehensive historical framework for the importance of IVI by charting the trajectory of modern endoscopy and highlighting the foundational role these internal viewing technologies play in contemporary precision medicine, particularly in the critical domain of cardiovascular care.

I. The Digital Dawn: Endoscopy’s Transformation in the 1980s and 1990s
The endoscopic revolution began in earnest with a single, profound shift in the way images were captured and transmitted. Prior to 1980, endoscopes relied on fiber optics, a technology that used thousands of delicate glass fibers bundled together. Each fiber transmitted a single pixel of light, collectively relaying a low-resolution, "honeycomb" patterned image. This method was mechanically fragile, prone to damage, and offered limited image quality, relying on an eyepiece for viewing.
The Charge-Coupled Device (CCD) Revolution
The pivotal moment arrived with the successful integration of the Charge-Coupled Device (CCD) into the distal tip of the endoscope. Developed in the 1970s but miniaturized and commercialized for endoscopy in the 1980s, the CCD is a photosensitive silicon chip capable of converting light into a digital signal. Placing this tiny camera at the end of the flexible insertion tube eliminated the need for the fiber-optic image bundle altogether.
This innovation ushered in the age of video endoscopy, transforming a solitary procedure observed through an eyepiece into a communal, high-quality viewing experience on a monitor. The benefits were instantaneous and profound: image resolution dramatically improved, eliminating the distracting fiber-optic pattern; the images were brighter and clearer, leading to enhanced detection of subtle lesions like early cancers or small polyps; and the devices became more durable and easier to sterilize.
This technological leap wasn't merely an upgrade; it was the foundation upon which all modern endoscopic therapy and minimal-access surgery would be built.
The Rise of Therapeutic Endoscopy
With vastly superior visualization, the medical community quickly recognized the potential to use endoscopes not just for diagnosis, but for treatment. The 1990s marked the era where endoscopy transitioned to therapeutic endoscopy. Engineers redesigned endoscopes to include larger working channels, allowing for the passage of sophisticated instruments.
This transition enabled complex, non-surgical interventions, dramatically reducing patient trauma and recovery times. Procedures like polypectomy (the removal of precancerous growths in the colon using a snare and electrical current) became routine, significantly reducing the incidence of colorectal cancer. Similarly, the development of specialized accessories allowed for complex bile duct interventions (ERCP, or Endoscopic Retrograde Cholangiopancreatography), control of gastrointestinal bleeding (hemostasis), and foreign body retrieval. The video endoscope became less of a viewing instrument and more of a precision surgical platform.

II. Setting the Stage for Intravascular Imaging: The Limitations of Angiography
To understand the historical importance of intravascular imaging (IVI), one must first grasp the limitations of its predecessor and competitor in vascular care: Angiography. For decades, angiography, which uses X-rays and injected contrast dye, was the gold standard for diagnosing coronary artery disease. It provided a powerful, two-dimensional silhouette of the flowing blood, allowing physicians to locate areas of narrowing, or stenosis.
The "Lumen Profile" Problem
The critical historical limitation of angiography is that it only visualizes the lumen, the internal channel through which blood flows. It is an image of the shadow of the plaque, not the plaque itself. This presented two fundamental problems:
1. Underestimation of Disease: Angiography often failed to accurately assess the true burden of atherosclerosis because the vessel can compensate for plaque growth by remodeling and expanding outward (Glagov phenomenon). A plaque that looks mild on X-ray might be extensive and vulnerable when viewed from the inside.
2. Inaccurate Sizing: When planning an intervention, such as placing a stent, physicians must know the precise diameter of the healthy portion of the vessel. Relying solely on the angiographic silhouette led to frequent instances of under-sized or poorly positioned stents, increasing the risk of later complications.
This diagnostic inadequacy created a compelling historical imperative for a technology that could provide a cross-sectional view of the vessel wall and plaque burden, establishing the need for Framework Point 1: Seeing Atherosclerosis.
III. The Advent of Intravascular Imaging: IVUS and OCT
Intravascular imaging effectively miniaturized the core principles of non-vascular endoscopy, focusing its powerful visualization capabilities on the coronary and peripheral arteries.
Intravascular Ultrasound (IVUS): The First Window (Late 1980s – 1990s)
Intravascular Ultrasound (IVUS) was the first widely adopted technology to overcome angiography's limitations. It involved placing a miniature, high-frequency ultrasound transducer onto the tip of a catheter, which was then threaded into the coronary artery.
IVUS provided a cross-sectional image of the vessel. For the first time, clinicians could measure the actual thickness and volume of the plaque, identify the composition of the arterial wall (calcified vs. soft plaque), and accurately determine the vessel’s true size. This marked a paradigm shift in understanding coronary disease. IVUS made it clear that plaque was often far more extensive than angiography suggested, and its use became invaluable for planning complex procedures and ensuring the mechanical success of balloon angioplasty and stenting.
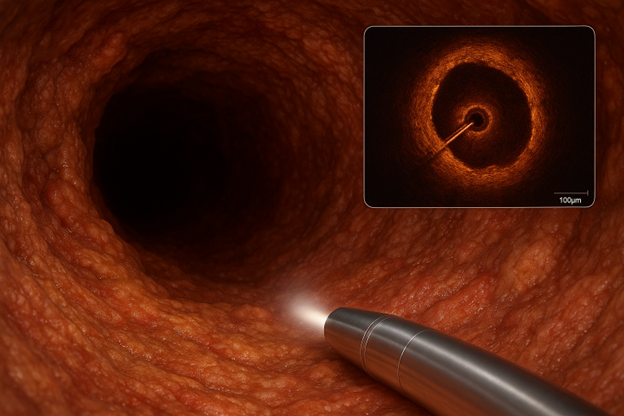
Optical Coherence Tomography (OCT): Microscopic Precision (2000s – Present)
While IVUS provided an excellent anatomical overview, the drive for greater resolution led to the development of Optical Coherence Tomography (OCT). This technology, drawing inspiration from fiber-optic communication and general endoscopic advances, employs near-infrared light waves instead of sound waves. It captures light reflected from internal structures to generate incredibly detailed images.

The resolution of OCT (typically 10−20 μm) is approximately ten times greater than IVUS. This microscopic capability established Framework Point 2: Guiding Intervention with Precision. With OCT, physicians could see features previously invisible: the thin fibrous cap covering a potentially rupture-prone plaque, subtle tissue prolapse, and, critically, the microscopic relationship between a newly placed stent and the vessel wall. OCT allows for the precise evaluation of stent expansion, its coverage of the lesion, and the presence of dangerous complications like malapposition (when the stent is not flush against the wall) or edge dissection, ensuring a much higher quality of procedural outcome.
IV. The Synergy of Endoscopy and IVI in Modern Medicine
The evolution of generalized endoscopy and specialized IVI are inextricably linked by shared principles: miniaturization, digital image processing, and therapeutic integration. Since the early 2000s, both fields have converged, often sharing similar fiber-optic delivery systems and digital processing hardware.
Endoscopy’s Advancements: Miniaturization and Robotics
General endoscopy continued its rapid pace of innovation:
● Ultra-Thin and Single-Use Scopes: The demand for access to smaller, more difficult-to-reach areas (like the smallest ducts or pediatric airways) led to the creation of ultra-thin endoscopes. Furthermore, concerns about infection control, particularly in high-risk procedures like bronchoscopy, spurred the development and widespread adoption of disposable, single-use endoscopes.
● Robotic Integration: The marriage of endoscopy and robotics, epitomized by the Da Vinci Surgical System, allowed surgeons to utilize endoscopic visualization while performing complex surgeries with enhanced dexterity and stability through small incisions. The endoscopic camera became the "eyes" of the surgical robot.
● Fluorescence and Narrow-Band Imaging: Advanced optical techniques were developed, such as Narrow-Band Imaging (NBI), which uses specific wavelengths of light to enhance the contrast of mucosal and vascular patterns, dramatically improving the early detection of superficial cancers in the GI tract.
Framework Point 3: Precision Medicine in Cardiology
The introduction and routine use of IVI technologies—IVUS and OCT—solidified Framework Point 3: Enabling Precision Medicine. Interventional cardiology is now less reliant on the subjective interpretation of X-ray shadows and more dependent on objective, quantifiable data derived from the vessel wall.
● Optimal Stent Strategy: IVI allows for accurate measurement of the minimum and maximum reference vessel diameters, ensuring the correct stent size is selected. Post-stent deployment, IVI confirms optimal expansion and coverage.
● Managing Complex Lesions: In cases of severe calcification, IVI guides the use of specialized tools like rotational or orbital atherectomy by precisely quantifying the degree and location of the calcified plaque.
● Long-Term Outcomes: Studies consistently show that IVI-guided stenting results in better long-term outcomes, including reduced rates of stent thrombosis (clotting inside the stent) and restenosis (re-narrowing), validating its clinical importance not just as a diagnostic tool, but as a therapeutic quality control instrument.

V. The Contemporary Frontier: Artificial Intelligence and Image Fusion
The latest chapter in the history of endoscopy and IVI involves their integration with computational power, pushing the limits of human perception and diagnostic accuracy.
Artificial Intelligence in Endoscopy
AI algorithms, leveraging the vast image datasets generated by digital endoscopes since the 1980s, are now capable of real-time image analysis. In colonoscopy, for instance, AI-assisted detection systems can instantaneously highlight subtle polyps or early neoplastic changes that a fatigued or distracted human eye might miss. These systems act as a constant, objective co-pilot, improving the overall quality and completeness of endoscopic procedures.
Image Fusion and Navigation
Modern procedures often involve combining the real-time, high-resolution view of the endoscope or IVI catheter with pre-operative volumetric scans (CT or MRI). Image fusion allows the endoscopist to see the internal view overlaid onto a 3D anatomical map, greatly enhancing navigational ability in complex procedures, such as bronchoscopy for peripheral lung nodules or complex neuro-interventions. This synergistic approach merges the macroscopic (from CT) and the microscopic (from the endoscope) into a single, comprehensive guidance system.
Conclusion: The Enduring Legacy of Internal View
The history of endoscopes since the 1980s is a testament to relentless technological innovation, transitioning from a simple visual aid into a sophisticated surgical and diagnostic powerhouse. This journey, propelled by the shift from fiber optics to digital chips, has delivered minimally invasive care to millions. The emergence of Intravascular Imaging—spearheaded by IVUS and perfected by OCT—is one of the most significant byproducts of this evolution.
The three historical pillars of IVI’s importance—its ability to see the true burden of atherosclerosis, guide complex interventions with micron-level precision, and enable a true paradigm of precision cardiology—have fundamentally reshaped the management of the world’s leading cause of death: cardiovascular disease. The continued convergence of advanced optics, miniature sensors, and artificial intelligence ensures that the next chapters of this history will focus on making internal visualization even more precise, intelligent, and universally accessible.
Frequently Asked Questions (FAQs)
1. What was the single most significant technological advance that allowed endoscopy to become "video endoscopy" in the 1980s?
The most critical technological advancement was the successful integration of the Charge-Coupled Device (CCD)—a miniature digital image sensor—onto the distal tip of the endoscope. Prior to this, endoscopes relied on fragile, low-resolution fiber-optic bundles to relay the image to an eyepiece. The CCD chip captured the image electronically, converting it to a video signal for display on a monitor. This shift from fiber-optic imaging to digital imaging dramatically improved image quality, resolution, and brightness, enabling multiple clinicians to view the procedure simultaneously, thus transforming it into a collaborative, teachable, and digitally recordable process.
2. Why was there a need for Intravascular Imaging (IVI) when Angiography already existed to view the coronary arteries?
Angiography (X-ray with contrast dye) only provides a two-dimensional shadow of the lumen profile (the hole through which blood flows). It cannot visualize the vessel wall itself. This limitation is crucial because coronary disease often involves plaque growing outward before it narrows the lumen significantly (Glagov phenomenon). Intravascular imaging, particularly IVUS (Intravascular Ultrasound) and OCT (Optical Coherence Tomography), allows clinicians to see a cross-sectional, 360∘ view of the vessel wall, accurately measuring the true plaque burden, identifying its composition, and precisely sizing the vessel for safe and effective stent placement. IVI established a need for precision medicine that angiography simply couldn't meet.
3. What is the main difference in technology and resolution between IVUS and OCT?
Intravascular Ultrasound (IVUS) uses high-frequency sound waves to generate a cross-sectional image. It offers deeper tissue penetration (up to 5-6 mm) and doesn't require clearing the blood from the vessel, making it excellent for assessing overall plaque burden and vessel size. Optical Coherence Tomography (OCT), conversely, uses near-infrared light waves. Because light is scattered by blood, OCT requires a brief flush of contrast to clear the vessel, but in return, it provides an axial resolution that is approximately 10 times higher (10−20 μm) than IVUS. This allows for microscopic visualization of subtle plaque features, stent struts, and precise healing patterns.
4. How did the development of the videoscope in the 1980s directly lead to the growth of therapeutic procedures?
The videoscope's superior visualization and high-definition display was the catalyst for therapeutic growth. When physicians could clearly and reliably see the target area on a large monitor, they gained the confidence and control necessary to pass complex surgical tools through the endoscope’s working channel. This directly enabled minimally invasive procedures like targeted polypectomy (removing polyps), endoscopic hemostasis (stopping bleeding), and the entire field of laparoscopic surgery, where the digital endoscope became the central camera guiding major abdominal operations.
5. What is the current "next frontier" of innovation in endoscopy and intravascular imaging?
The current frontier is the integration of Artificial Intelligence (AI). AI algorithms are being trained on vast image datasets to serve two primary functions: Computer-Aided Detection (CADe), which highlights subtle lesions (like early polyps or vulnerable plaque) in real-time to prevent human error or fatigue; and Computer-Aided Diagnosis (CADx), which can characterize the nature of a lesion (e.g., neoplastic vs. inflammatory) or assess the completeness of an intervention with objective, quantitative metrics. This fusion of optics and computation is poised to further enhance diagnostic accuracy and standardize the quality of endoscopic procedures globally.